2022-5-25
Abstract
Background & aims: Colonoscopy for colorectal cancer screening is endoscopist dependent, and colonoscopy quality improvement programs aim to improve efficacy. This study evaluated the clinical benefit and safety of using a computer-aided detection (CADe) device in colonoscopy procedures 本研究评估了在结肠镜检查程序中使用计算机辅助检测 (CADe) 设备的临床益处和安全性.
Methods: This randomized study prospectively evaluated the use of a CADe device at 5 academic and community centers by US board-certified gastroenterologists (n = 22). 多中心 Participants aged ≥40 scheduled for screening or surveillance (≥3 years) colonoscopy were included; 【排除标准】exclusion criteria included incomplete procedure, diagnostic indication, inflammatory bowel disease, and familial adenomatous polyposis. Patients were randomized by endoscopist to the standard or CADe colonoscopy arm using computer-generated, random-block method. 【终点】The 2 primary endpoints were adenomas per colonoscopy (APC), the total number of adenomas resected divided by the total number of colonoscopies; and true histology rate (THR), the proportion of resections with clinically significant histology divided by the total number of polyp resections. The primary analysis used a modified intention-to-treat approach.
Results: Between January and September 2021, 1440 participants were enrolled to be randomized. After exclusion of participants who did not meet the eligibility criteria, 677 in the standard arm and 682 in the CADe arm were included in a modified intention-to-treat analysis. APC increased significantly with use of the CADe device (standard vs CADe: 0.83 vs 1.05, P = .002; total number of adenomas, 562 vs 719). There was no decrease in THR with use of the CADe device (standard vs CADe: 71.7% vs 67.4%, P for noninferiority < .001; total number of non-neoplastic lesions, 284 vs 375). Adenoma detection rate was 43.9% and 47.8% in the standard and CADe arms, respectively (P = .065).
Conclusions: For experienced endoscopists performing screening and surveillance colonoscopies in the United States, the CADe device statistically improved overall adenoma detection (APC) without a concomitant increase in resection of non-neoplastic lesions (THR).
简评:前瞻性多中心CADe研究,1440例,腺瘤/肠镜率;
2022-6-30
摘要:
Introduction: Computer-aided detection (CADe) helps increase colonoscopic polyp detection. However, little is known about other performance metrics like the number and duration of false-positive (FP) activations or how stable the detection of a polyp is.
Methods: 111 colonoscopy videos with total 1,793,371 frames were analyzed on a frame-by-frame basis using a commercially available CADe system (GI-Genius, Medtronic Inc.). Primary endpoint was the number and duration of FP activations per colonoscopy. Additionally, we analyzed other CADe performance parameters, including per-polyp sensitivity, per-frame sensitivity, and first detection time of a polyp. We additionally investigated whether a threshold for withholding CADe activations can be set to suppress short FP activations and how this threshold alters the CADe performance parameters.
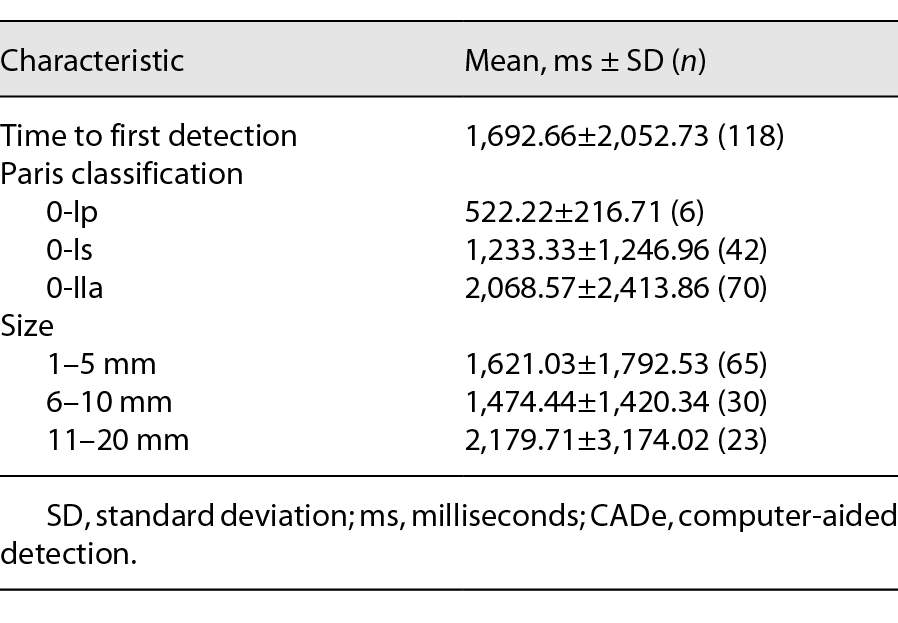
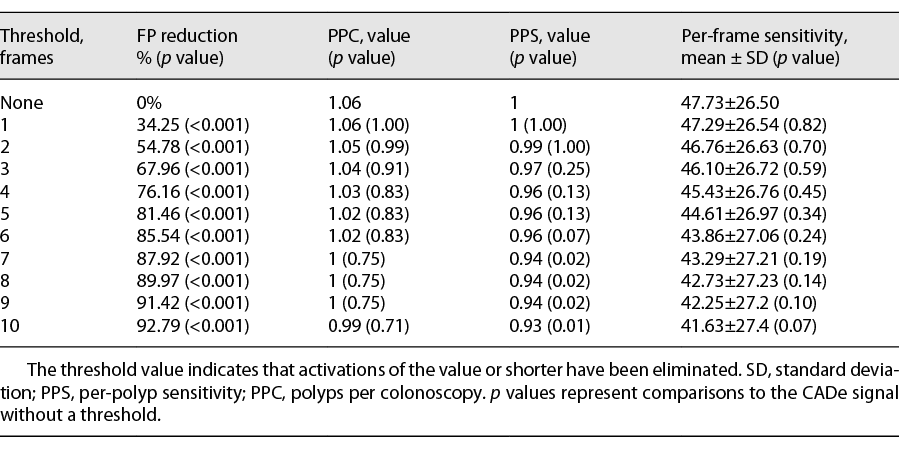
Results: A mean of 101 ± 88 FPs per colonoscopy were found. Most of the FPs consisted of less than three frames with a maximal 66-ms duration. The CADe system detected all 118 polyps and achieved a mean per-frame sensitivity of 46.6 ± 26.6%, with the lowest value for flat polyps (37.6 ± 24.8%). Withholding CADe detections up to 6 frames length would reduce the number of FPs by 87.97% (p < 0.001) without a significant impact on CADe performance metrics.
Conclusions: The CADe system works reliable but generates many FPs as a side effect. Since most FPs are very short, withholding short-term CADe activations could substantially reduce the number of FPs without impact on other performance metrics. Clinical practice would benefit from the implementation of customizable CADe thresholds.
简评:通过对GI-genius的回顾性逐帧分析,对于111个肠镜视频,平均每个肠镜出现了101±88个假阳,每个假阳的平均持续时间是135ms,占退镜时间的2.48%(13.61s)。绝大部分假阳性出现1-3帧,1.6 ± 2.1% of the frames with polyps contain this distraction。GI-Genius的逐帧灵敏度为46.6 ± 26.6%;扁平息肉检出率37.6 ± 24.8%显著更低;右半结肠检出率显著更低(43.56 ± 25.04% vs. 53.43 ± 26.00, p = 0.017);FDT(息肉首次出现到第一个真阳出现):平均1,692 ± 2,052 ms。
不同阈值效果:(6帧时效果较好)
分析方法:如果边界框与可见的息肉接触,则认为是 TP,无论病变区域被覆盖多少。直肠乙状结肠的小增生性息肉被排除在分析之外。在具有可见息肉的帧中没有边界框被认为是假阴性。